- Be up-to-date with vaccinations, including boosters, as appropriate.
- Rapid test and self-monitor immediately before and during an event.
- Properly wear a mask while meeting with others or in public areas.
- Isolate at the sign of any symptoms.
- Wear my pledge pin at HPC events.
Coronavirus Disease 2019 (COVID-19) is a mild to severe respiratory disease that is caused by the SARS-CoV-2 virus (Severe Acute Respiratory Syndrome, Coronavirus, version 2). Coronaviruses are a class of viruses with ribonucleic acid genomes (RNA) and a characteristically shaped “Spike” protein on its surface resembling a corona or chevron. SARS-CoV-2 uses these spike proteins to gain entry into host cells that express the angiotensin converting enzyme 2 (ACE2) receptors on their cell surface. ACE2 is an enzyme that generates small signaling proteins that are created by cutting the larger protein, angiotensinogen, in specific places. Those small proteins go on to regulate functions in the cell. Many cells in the body express this receptor, including cells lining the lungs, throat, nasal passages, heart, blood vessels, kidneys, adipose tissues (fat), selected neural tissues, and cells lining the gut. ACE2 is a critical receptor in the circulatory system that regulates blood pressure and inflammation, without which those processes can continue unchecked and lead to damage to those tissues.
SARS-CoV-2 infects these cells, deposits its RNA genome into the cell, converts it to a DNA strand (reverse transcription), and utilizes the cell’s machinery to replicate thousands of new viruses that are secreted from the cell back out into the body. Because COVID-19 hijacks cells of this type, extensive tissue damage can occur in the tissues listed above, causing many of the common symptoms and long-term effects commonly associated with this disease. Because the virus can replicate so quickly in the body, it can cause a massive inflammation response that can lead to high fevers, difficulty breathing, and multiple organ dysfunction, which often leads to death in individuals that are susceptible to that combination of responses to the virus.
One important feature of all coronaviruses is their ability to quickly mutate in a manner that evades any prior immunity against infection that may have been acquired through infection or vaccination. If left unchecked and uncontrolled, this rapid mutation rate cannot be overcome by population immunity (no herd immunity), thus causing new strains of the virus to emerge faster than immunity can be gained. Since the spread and containment of COVID-19 have gone completely unchecked, it continues to become more and more infectious, resulting in a virus that is so efficient at infecting our cells that it takes a very small amount of the virus very little time to cause infection.
Over the last three years, hundreds of studies have proven countless times that SARS-CoV-2 is an airborne virus that can hang in the air in aerosols expelled from the lungs of people infected with the virus. The virus can live for up to three days floating in the air and can infect anyone that walks through the aerosols and exposes their respiratory system to enough viral particles to overcome initial immune responses in those tissues.
It is important to note that since the virus continues to mutate and become better at infecting humans, it now takes a very small amount of virus less than 15 seconds to infect a person who inhales the particles. The original virus (originating from bats) took nearly 15 minutes to infect humans by comparison.
SARS-CoV-2 omicron strains BA.5 and BA.2.75 are now some of the most infectious human diseases in recorded history.
This question is asked all the time, and the truth is that the current state of the pandemic has been messaged this way. However, the virus is not yet endemic and the pandemic is not over yet. In order for the virus to be endemic, the population must have enough immunity to the disease that each person infects less than one other person, which would prevent a large outbreak of the disease from ever happening again. This is not currently the case, as most people are still infecting several to 10s of other people, keeping the transmission high and the number of people infected at any one time very high. It is estimated that, at the current rate of mutation and lack of large-scale mitigations, we likely have up to two years before the pandemic can be declared over and the virus endemic. Importantly, it is possible that this state will never be reached, and we will have the current level of infection until the planet collaborates on truly getting the disease under control.
Additionally, while the vast majority of cases of COVID-19 have mild to light symptoms currently, the virus itself is quite dangerous to certain portions of the population (immunocompromised, unvaccinated and previously uninfected people, elderly people, etc.), and there’s no guarantee that future variants won’t emerge as largely harmful. The disease has become largely mild due to the massive partial immunity acquired by the global population, both through vaccination and through infections. However, as was covered in the last question, this virus evolves quickly and conceivably has the capability to render any existing immunity useless in future infections, which would result in the disease being as dangerous as it originally was. The chances of this happening are relatively low, but it’s important to note the possibility when measuring your individual risk.
The final issue with the “COVID is no big deal” line of thinking is that there are still a very large number of unknowns associated with a COVID infection. The biggest question is the condition known as long COVID. In 30% of all cases (not just in any specific part of the population), long-lasting symptoms develop that can, at a minimum, reduce someone’s quality of life and, at a maximum, completely disable them. The average length of long COVID is 8 months, with some cases still continuing three years after the original infection. Very little is known about why this happens or how to treat it, but a wide array of research studies are underway to try to find out.
Yes, they work quite well against the virus. All of the vaccines currently in circulation throughout the world (over 20 different formulations and types) were targeted to the original strain of the virus from 2019. If that virus were circulating, the vaccines would all be very effective at preventing infection, symptoms, and severe disease. Since the virus has mutated very far away from that original strain, the vaccines are less effective at preventing infections and symptoms but are still quite effective in preventing severe disease.
The vaccines protect against severe disease by training your immune system to ramp up and mount a specific attack against the viral particles that do not mutate but are not accessible to the immune system upon infection. They are only accessible as cells are secreting replicated viral particles, thus allowing vaccination to reduce the degree of infection and vastly reduce the chances of developing severe disease.
Unfortunately, no. Like most risky situations, multiple layers of mitigation are needed to reduce the risk of infection from this disease. One way to think about these layers is to consider the “Swiss Cheese Model” (see image below). In this model, each slice of cheese has holes in it. The virus can pass through these holes, but some of it is blocked at each layer. If another slice with different holes is after that, then more viruses are blocked, and so on. Each slice of cheese represents a type of mitigation that can collectively reduce the risk of infection and severe disease.
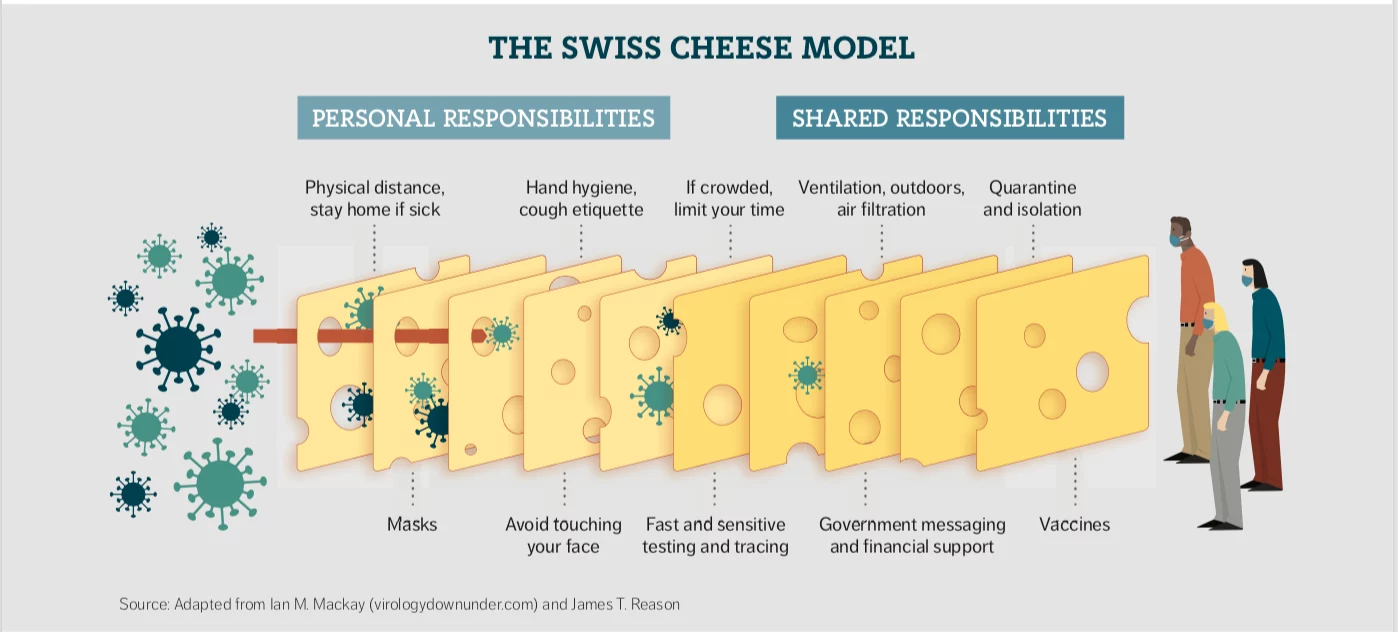
Source: https://www.infectioncontroltoday.com/view/wiss-cheese-model-how-infection-prevention-really-works
Note that the above image is from 2020, so many of the assumptions in the image have changed. The main mitigations to focus on now are vaccination, masking, testing, isolation, and ventilation. These are discussed further in other FAQ sections below.
No, there is no truth to claims that mRNA vaccines are dangerous. Most people are skeptical of new technologies, especially medical technologies. Plus, the way mRNA vaccines work is complex and confusing and has generally not been well explained to the public leading to a lot of skepticism about whether they work and are safe. Here, we go through a VERY brief explanation of how they work.
Above, we discussed the immune-evading capabilities of SARS-CoV-2. One way that the virus evades the immune system is by cloaking the spike protein in slippery sugars called glycans. These sugars keep much of the spike protein from being exposed to the immune cells that would recognize and create antibodies against foreign agents in the body, slowing the immune response and allowing more viruses to infect more cells before the immune system can mount a response. Since the spike protein is how the virus infects cells, antibodies to it would prevent infection by binding to the spike protein and targeting it for destruction.
mRNA vaccines work by delivering thousands of strands of RNA into muscle and lymphatic cells. These mRNA strands instruct those cells to make thousands of uncloaked spike proteins that are then secreted into the bloodstream. The mRNA sequence was designed by the manufacturers to be a stabilized version of the spike protein that always has the ACE2 binding site exposed so the immune system can create antibodies to that and other sites on the protein. Those antibodies can then bind to the real spike proteins on viruses that have entered the body, both preventing widespread infection of cells and shutting down any infected cells before they can exponentially infect other cells, thus preventing the infection from taking hold.
mRNA stands for messenger RNA. There are many different kinds of RNA in our cells that have many different functions. mRNA is created from the DNA in each cell and tells the cell how to make the proteins that allow it to perform its intended functions. Because of the natural mechanisms of mRNA processes in cells and the fact that RNA is much less stable than DNA, mRNA from the vaccines within the cells only lasts 72 hours before it is broken down by the cell, thus halting the creation of spike proteins within those cells. Once the mRNA levels reach zero, the cell goes back to its normal state, and no more spike protein is made. The circulating spike proteins are also purged from the body through natural excretion processes in that same time frame, but not before they’ve taught your immune system how to defend against SARS-CoV-2 without actually being infected.
There is very little danger to these vaccines. In many ways, they are much safer than traditional vaccines, some of which use non-replicating living viruses to evoke the immune response. Full viruses can cause all sorts of complications, just like the full replicating versions, and can cause many unforeseen adverse reactions in the body. The number of adverse reactions possible in the mRNA vaccines (which use lipid nanoparticles to deliver the mRNA, the same material that makes up the membranes around your cells) is far lower than in the old technologies.
Additionally, over three billion people worldwide have received mRNA vaccines against COVID-19. If there were significant adverse effects from the vaccines, we would know by now, given the very large proportion of the population that has been inoculated.
There are currently no known biologically plausible long-term effects of receiving mRNA vaccines. Much of the misinformation that people have heard along these lines claim that these vaccines alter your cells’ DNA, thus leading to permanent long-term effects from the vaccines. This is not true and cannot occur from the mRNA delivered by the vaccines. RNA is not DNA, and our genomes are composed of DNA. The normal biological process in cells starts with “transcription,” in which genes encoded in your DNA are read and transcribed into mRNA strands that are then exported from the cell’s nucleus into the cytoplasm. The mRNA is then read by other proteins (ribosomes) and translated into proteins that are then further modified to the final active proteins and enzymes that perform all functions within your body.
This process does not operate in reverse within our cells naturally. There are classes of viruses (i.e., retroviruses) that deliver mRNA, reverse transcribe them to DNA, then incorporate them into the host cell genome, thus making that cell a permanent virus production house until the cell dies or is destroyed. That process requires foreign mechanisms to be present in our cells, and the mRNA vaccines do not employ those mechanisms.
So, the only long-term effect of mRNA vaccines is the same as all vaccines: the immune system is taught how to defend against those agents for a long period of time, if not permanently (depending on the type of immunity gained during exposure).
Yes, it’s important to still be safe. The SARS-CoV-2 virus isn’t like most other diseases we’re used to. As was explained in the “What is COVID-19?” question above, these viruses have a very high rate of mutation that allows them to escape prior immunity gained by individuals. And, the pace of mutation and spread of new variants is faster than we can adapt to them. As a result, prior immunity from prior variants does very little to prevent infection with from a new variant.
So, while prior immunity and vaccines can help keep you from getting very sick from the virus, you can almost continuously get reinfected as each new variant emerges and spreads through the population. So, doing your part to slow the spread while also protecting yourself from reinfection by taking the pledge is still important even if you’ve already had a COVID-19 infection.
Masking has become a highly controversial issue in American society. The controversy largely stems from extremely poor communication by the federal government to the population about how they work, why they work, and in what situations they are and are not useful. Additionally, the messaging has changed over time without explanation, leading people to believe that masks don’t work. Finally, most Americans are very resistant to wearing masks since they are slightly uncomfortable and inconvenient, leading to large-scale resistance to compliance with mask-wearing.
The truth is that masks work quite well in limiting the transmission of all airborne diseases, including COVID-19. However, the type of mask used is very important, and the degree of mask-wearing makes a huge difference in the limitation of transmission.
When the pandemic first emerged, the SARS-CoV-2 virus was adapted to bats, not to humans. That meant that it took a lot of virus being exposed to your airways for a long period of time to become infected. During that time period, anything sitting in front of your mouth and nose would significantly slow the amount of virus you exhaled (if you were infected) and limit the amount you inhaled enough to significantly reduce the risk of becoming infected, even though some masks (like cloth masks and very leaky surgical masks) are only 50% effective overall.
Masks work best when everyone is wearing them because the effect is additive. Having anything in front of your face if you are coughing or sneezing will limit the distance that infected particles will travel. If two people are in a room and each is wearing a mask that is 50% effective, the combination of the two masks will make them 75% percent effective. If two people are wearing masks that are 95% effective, the combination will be 99.96% effective at blocking transmission. Since most people have given up wearing masks, it is very important to understand how to properly wear a mask to protect yourself from those that are not wearing masks.
As we’ve allowed the virus to mutate, it has continued to become better adapted to human physiology, and we are now at a stage of the pandemic where the virus takes only a few seconds and a very small amount of time to infect a new host. As such, only high-filtration masks (N95, KN95, KF94, P100) significantly reduce the chances of you becoming infected or infecting others if you are already infected. The most common and most effective mask is the N95, which has straps that wrap around your head and if worn properly, seals against your face so that all air being inhaled or exhaled travels through the mask’s fibers. Masks with ear loops (KN95, KF94) do not seal as well to your face and are not quite as effective as a result. P100 masks and the like have elastomeric seals against your face, are generally plastic and have filters that attach to the base of the mask. These can be 100% effective in blocking the virus but are quite uncomfortable and look like gas masks.
More discussion of how masks can stop viruses can be found in the next question.
As was mentioned above, how masks work is complicated, nuanced, and has been poorly explained to the public. If you think of masks as being a single plane with small holes in it that each of the viral particles can easily slip through, this notion would be correct. However, that is not at all the case. The high-filtration masks listed above, specifically N95 and KN95 masks, use a combination of properties to filter out organic substances as they pass through the mask material.
First, these masks are composed of many interlaced layers of fibrous material that form a very complex path for macromolecules and microscopic life forms to get through (i.e., viruses and bacteria). This alone traps a large portion of viruses as they pass through, as well as catches the water microdroplets (aerosols) in the air and coming from your lungs in which the viral particles are suspended. While this complex pathway through the mask materials can block viruses, water droplets, and bacteria, it very minimally restricts the flow of air through the material. Yes, it is slightly more difficult to pull and push air through them, but the effect is minimal. Additionally, small organic compounds like oxygen and some odor-causing small molecules can pass through just fine, which is why you can smell some things through the mask even though it is working properly.
Second, these masks are composed of fibers that are positively charged. The vast majority of organic materials share an overall negative electrostatic charge, including viruses. So, the additional positive charge in the mask materials captures viruses more strongly using the opposite charge they carry to hold them in place, rather than just relying on the viruses to stick to pockets in the materials. This combination of factors is how a thin fibrous mask can effectively block 95% of viruses passing through the mask materials.
As was mentioned above, the fit of these masks to your face is critical to accomplishing the 95% effectiveness rating. There are many videos online that demonstrate in just a few minutes how to properly wear an N95 or KN95 mask. If you are someone who is willing to wear masks, we highly recommend that you watch these videos.
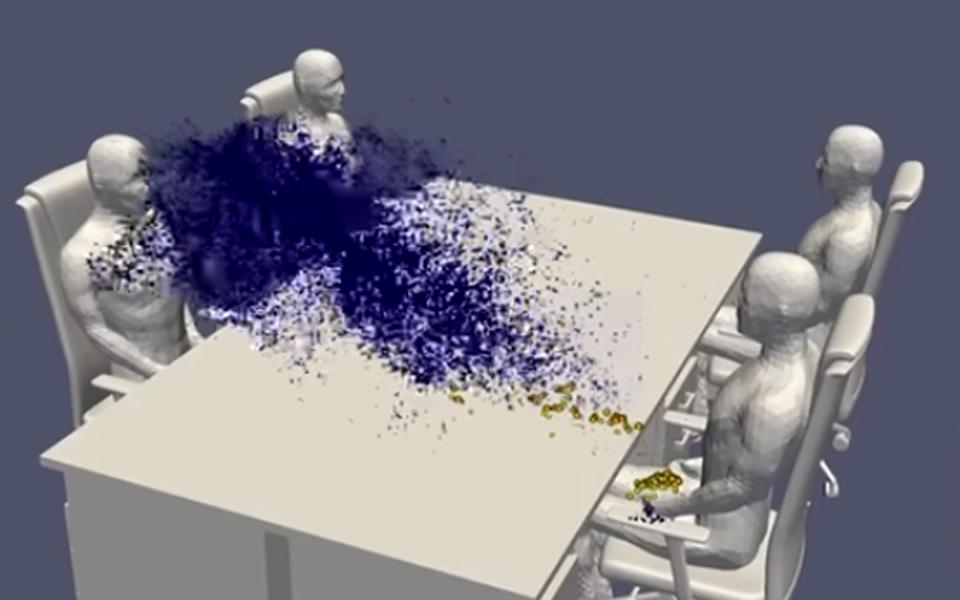
Specifically for the HPC community, it is important to point out that much of the effective research for masking was simulated on the very supercomputers we use and pay attention to. The first very effective simulation of aerosol movement in rooms, with and without masks of various types, was performed on the famed supercomputer, Fugaku of the Riken Institute in Japan, which also held the #1 spot on the Top500 list for multiple years. An image from that research is shown below and videos from those simulations can be found in the link above.
Unfortunately, the CDC guidelines do not make sense for the current state of the pandemic. Their recommendations are geared towards a virus that is endemic and a community that has a large degree of active immunity to the disease. Neither of these conditions is true, and those guidelines are perpetuating the pandemic longer than it needs to be. The science known to date clearly shows that completely asymptomatic people can be infected and actively spread the virus. Additionally, people whose symptoms have resolved can still be infectious (and test positive by rapid antigen test) up to 10 days after being infected. Additionally, the CDC states that people are less likely to be contagious after 10 days of infection, which is also usually true. The CDC also recommends that after five days, the person wear a mask until day 10, but the lack of compliance means this will likely not happen. Since public health related to the pandemic has become a politically charged issue, the CDC has not updated its recommendations to better reflect the science and support the reduction of transmission of COVID-19.
A set of procedures more aligned with the science would be as follows: 1) test if you feel sick or have been exposed to someone who is positive, 2) isolate until symptoms resolve and the person tests negative on a rapid test (which can take up to 14 days). If one must leave isolation, they should wear a properly fit N95 mask to protect others from getting infected by them, and they should return to isolation when possible. Additionally, infected people should gather while masked in well-ventilated areas or in vehicles with ample outside airflow moving through the cabin. This combination of mitigations would vastly reduce the infection rate in the US. If combined with a higher degree of compliance with mask-wearing, we could likely end the pandemic in a much shorter timeframe without extensive lockdowns or limiting people’s day-to-day lives.
Absolutely. COVID-19 is an airborne disease that is carried in suspended aerosols for long periods of time. Moving air around and passing it through effective building filters (like MERV-12/13 or HEPA-rated filters) and/or replacing it with fresh air will GREATLY reduce the spread of the virus. This is why gathering outdoors is so much safer than being inside because there is no better ventilation than being outside. Unfortunately, with the current level of infectiousness of SARS-CoV-2, even outdoor gatherings can cause transmission if people are very close together or there is very little if any, wind to move the air around.
One thing you can do to judge the risk of a place you’re in is to see if you can feel moving air. If the air is moving in a perceptible manner, the risk of transmission is reduced. Without understanding the specifics of the ventilation system, it is impossible to predict the degree of risk reduction, but as a rule of thumb, any ventilation is better than none (especially in combination with high-filtration masks and vaccinations).
One way organizations can help is to have in-room HEPA filters and CO2 monitors that show that air is being filtered. Stagnant air collects CO2, and a CO2 monitor can show the degree of air changeover. These monitors are inexpensive and very effective measures of air recycling in an enclosed space. Additionally, temperature checks upon entry can catch unknown or unreported cases (although the newest strains don’t always cause a fever).
Since the US has largely eliminated or banned most sensible COVID-19 mitigations and has stopped acknowledging the pandemic, it is increasingly challenging to social distance. That being said, adequate filtration combined with a population that has tested prior to gathering and is wearing masks, largely reduces the risk of transmission to extremely low levels. If these conditions are all met, social distancing isn’t necessary. Ventilation and testing right before an event are the best paths to being able to hold a normal gathering. Adding masks makes it that much safer for everyone involved in the event that someone attending is shedding large amounts of the virus unknowingly.
This is one of the topics that have been most poorly communicated to the general public throughout the pandemic. In December 2019, we were exposed to a virus that had never been seen in all of human history. It was a truly novel virus, and we knew absolutely nothing about it. We knew it was somewhat similar to the original SARS virus from 2012, but that’s where the similarity ended. Science works by testing hypotheses and seeing if they hold up while answering why or why not during the study. As we learn more and more, what we know changes, and with a disease as widespread as COVID-19, that is still the case in late 2022.
Science is a constantly changing field. In the beginning, when lockdowns first occurred in the US, certain statements were made in a manner that implied that the pandemic was a simple situation that we knew everything about. Nothing could be further from the truth. Those communicating to the public at the time also understood this fact, so the choices of wording were even more confusing.
As our understanding of the virus, how it transmits, the disease state, and how to treat it evolved, the guidance and recommendations also changed. Since the fluid nature of our understanding of the virus was never explained to the public, along with the very nuanced set of conditions that change the things you should do during the pandemic, the public was highly confused when the government kept changing their story and speaking in absolutes when there was nothing absolute about this situation. Eventually, people got angry and fed up and decided that the government didn’t know what they were doing. This resulted in an increased political alignment on how to (or how not to) accommodate the pandemic, and resulted in a population that simply threw their hands up, went back to normal, and stopped believing the science and the communications coming out about it.
Science is ever-changing. We have learned a lot about this virus, possibly more than we’ve known about other viruses. In fact, we’ve learned so much that we now know much more about how disease is transmitted in general, not just for COVID-19.